Stroke: Update 2018
May 1, 2019•900 words
https://mdstudent.kku.ac.th/Database/files/Clinic/Medicine/All%20about%20stroke.pdf
- NIHSS evaluation q 4 hr ระหว่าง admit ก็มา จาก พี่ MH
Airway
- GCS <= 8 need ETT + MV
Breathing
- SpO2 >= 94 perecent (ไทยเขียน 92 จ้า?)
Circulation
- To Preserve cerebral perfusion
- IV Fluid Non-dextrose Hydration rate maintenance
- หลีกเลี่ยงการให้ ที่มีน้ำตาลหรือ free water เนื่องจากอาจทำให้เกิดภาวะ
สมองบวมมากขึ้น
Physiologic Control
| BP |
|
| BT | Central fever |
| PR | Monitor bradycardia for Cushing triad, Brain herniation |
| RR |
Blood Sugar Control
- Hyperglycemia
- <evidence from NICE sugar study: critical for non-DM>
- best to keep 140-180 @-@
- 110-140 acceptable
- keep<110 increase mortality
- 80-140 ??? เล่ม มข เขียนทำไมมม
- Hypoglycemia
- not <60
Food
- NPO เว้นยาได้ ถ้า
- rTPA 24 hr
- large infarction
- ซึม
- Infratentorial infarction (cerebellum, brain stem)
http://pni.go.th/cpg/sft-2007.pdf ดูหน้า 15
Monitor IICP and Brain Herniation
- Risks
- Hemorrhage
- Brain edema
- Large Infarction
- Prevent
- Elevate head สูงกว่าระดับหัวใจประมาณ 30 องศา
- หลีกเลี่ยงการกระตุ้นผู้ป่วยที่จะส่งผลให้เกิด Valsalva responses
- Prophylactic craniotomy ?
- Observe Clinical
- GCS drop, unequal pupils, hemiplegia, Cushing's triad
- Follow up imaging
- At 24-48hr ?
- At 1wk ?
- Before starting Anti-Coagulant ?
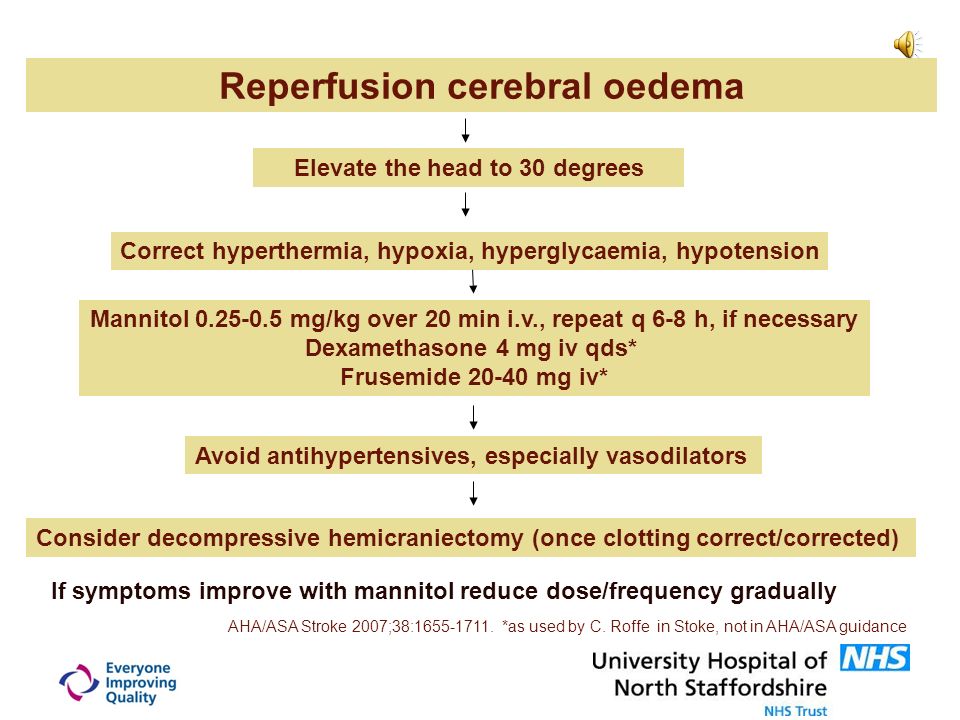
- Management
- Medical
- monitor: Cushing reflex, unequal pupils dilated, EKG, SpO2
- ยกหัว 20-30 องศา
- Maintain Normovolemia - Correct Hypovolemia !! ยากล่ะ
- Furosemide?
- A brief period of Hyperventilation (15–30 min) with a PaCO2 target of 30–35 mmHg [ref]
- Mannitol <SE: rebound หลังหมดฤทธิ์ ต้องผ่าแก้เสมอ>
- LD 1-1.5 กรัม/กิโลกรัม และ 0.25-0.5 กรัม/กิโลกรัมในกรณีที่ให้ซ้ำ
- 20% Mannitol: 0.25-0.5g/kg= 1.25-2.5ml/kg
- 20% Mannitol: 5ml/kg (250ml) IV drip in 1hr LD
- Dexa: AHA ไม่ให้นะจ้า แต่มีคนให้
- Surgical: Craniectomy

Secondary Prevention (Prevent Recurrence)
- Antiplatelet
- For General
- ASA life long
- CHANCE study: For High risk TIA or Minor stroke NISHH <4
- Dual Antiplatelet
- Anti-coagulant
- For cardioembolic stroke
- DO NOT GIVE IF LARGE INFARCT? - High Hemorrhage Risk
- Manage AF with stroke
- CHADVASC >=2
- Valuvular AF
- High-intensity statin
- Benefit to all patients no matter how lipid level is
- Atorvastatin 40
- Rosuvastation 20
- Work Up Co-Morbid
- DM: Blood for HbA1C, FBS
- Supplement
- Vitamin B, Folic acid
- Benefit for lowering homocysteine level associated with increased recurrent stroke
Rehabilitation
- Prevent joint stiffness, lung atelectasis, bed sore
Aspiration Prevention
- Dysphagia screening
- Gag reflex
- Swallowing test
- If risk aspiration - elevate head of bed, NG tube feeding
Stroke in the Young <45 years work up
- Atherosclerotic risks
- Arteritis
- VDRL
- ESR,CRP
- CNT Dz
- ANA screen
- Thrombophilia
- Anti Phospholipid antibody
- Protein C, S, Antithrombin III, Factor V Leiden
- Homocysteine level
- Host
- AntiHIV
- Coag
- Vascular study
| Imgur จาก Thai CPG Hemorrhagic Stroke(pdf) ดีมากๆ อ่านภาคผนวกดู |
Protocol MNKH: http://www.medkorat.in.th/admin/ckfinder/userfiles/files/VERSION%20I%2023%20SEP%202016.pdf |
|
